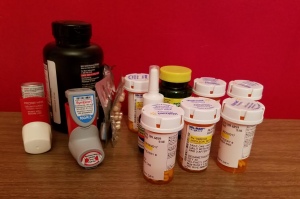
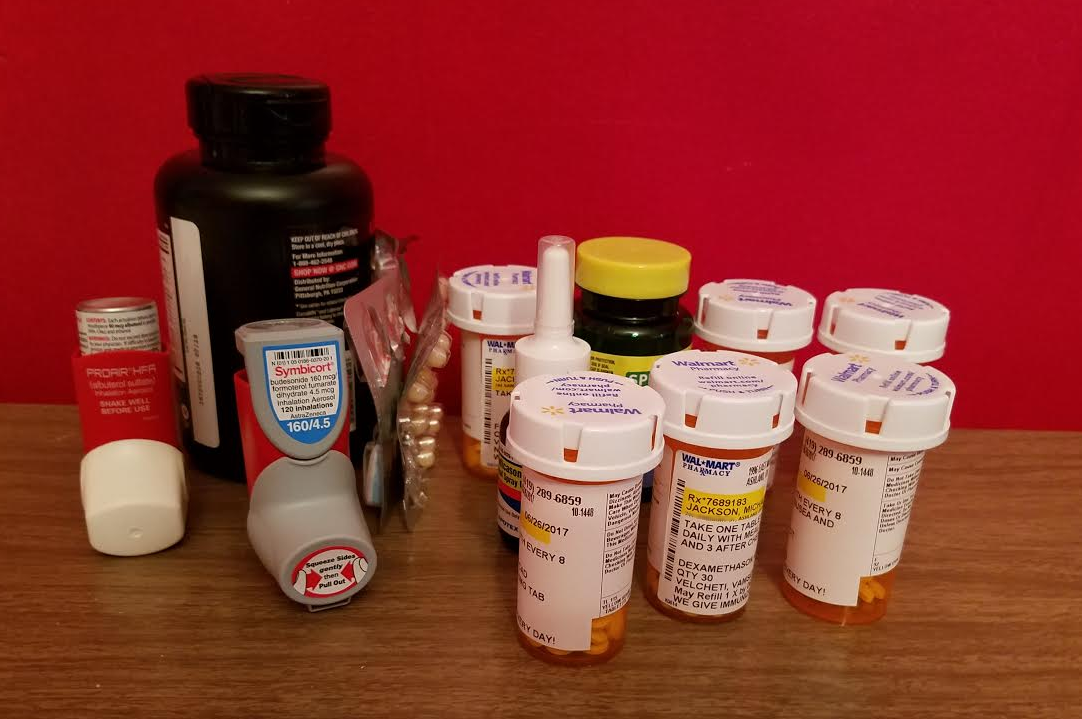
 Every morning, he looks at the ever-expanding collection of medicines on the breakfast table, and screws up his courage.
Every morning, he looks at the ever-expanding collection of medicines on the breakfast table, and screws up his courage.
His lung tumors and swollen lymph nodes are pressing on areas of his larynx and vocal folds, as well as on his esophagus. Not only can he not ever clear his throat or get a productive cough (take a moment and envision going through that 24/7), but now he is having trouble swallowing. Taking these pills each day is getting to be an uphill struggle.
But he still found the humor to laugh about his clumsiness with attempting to put some cans of pop in the fridge and scraping his arm against the cardboard packaging. He proudly showed me yet another bandage on his arm. The man simply cannot stay out of trouble.
So, the public service announcement…
Did you know that lung cancer is the #1 cancer killer of both men and women? According to the American Cancer Society, lung cancer kills more people each year than breast, prostate, colon, liver, kidney and melanoma cancers combined. We have massive awareness campaigns for these other types of cancers, but where is the ribbon for the #1 killer? I’ve never seen a mainstream push for screening for lungs. Shall I start one? I wonder if the Thriller would volunteer to be the poster child. Hmmm…
You may ask: What is the screening process for lung cancer? Well, that’s where it can be a bit tangled and dark. Suffice to say that I know an encyclopedia’s worth of stuff about lung cancer today, compared to what I knew in May. As you might imagine, I’ve done little else with my spare time except read up on it:
- It often takes 10-20 years or more for lung cancer symptoms to manifest. I have read many personal accounts of people who never had any symptoms (persistent cough, weakness, breathlessness, constant fatigue, swelling of extremities or lymph glands, vocal cord paralysis, trouble swallowing, hoarseness, rapid weight loss, wheezing, chronic bronchitis) until their cancer was already in its advanced stage — which is exactly what happened in our house.
- CT scans are the best screening for lung cancer, but they are not without their problems. According to cancer.org, the trouble is that computed tomography x-rays often find abnormalities that look like cancer, but aren’t. This can lead to biopsies and other tests that potentially lead nowhere. Still, if it’s the best you have and you want to know, I’d go for it. I’m going to — believe it.
- Are you “high risk?” Then get thee to the doctor for a screening appointment. To be in the high risk category, you must be aged 55 to 74 years, have a smoking history equivalent to a pack a day for 30 years, and currently smoke or have quit within the past 15 years. The Thriller quit smoking in 2010, at age 58. That’s about when his COPD began to kick in. What we thought was the slow progression of emphysema was actually the rising onset of lung cancer.
- Lots of people who get lung cancer have never smoked. Just because you’re not high risk doesn’t mean you’re in the clear. I think *everyone* should be screened for lung cancer, right along with getting the mammograms and PSA counts and pap tests and colonoscopies.
I wanted to know some history of the disease, especially as related to cigarette smoking. Here’s the initial trend, from the Lung Cancer Guidebook:
Lung cancer is a relatively new problem for human beings. In the early 1900s, lung cancer was extremely rare. Although people have used tobacco for centuries, until the early 1900s, it was most often smoked with a pipe, in a cigar form, or chewed. The machines to mass-produce cigarettes were invented in the 1880s, but it was not until after World War I that cigarette smoking became prevalent in the United States.
During the war, American soldiers were given free cigarettes donated by tobacco companies to the U.S. military. Many soldiers left the military with a lifelong addiction to the nicotine in tobacco products. At that time, the medical community did not realize the long-term impact of cigarette smoking on health.
So here we are, a hundred years later, seeing the avalanche finally letting loose. It’s time to bring lung cancer forward on the parade route, not to supplant the other kinds of cancers out there, but to march on the same front line. Consider me endowed with a new purpose.
Much love,
#teamthriller

 While talking over coffee this morning, we realized that the number 31 has more than a passing significance for us. (As we discussed it, I happened to glance at the microwave. haha)
While talking over coffee this morning, we realized that the number 31 has more than a passing significance for us. (As we discussed it, I happened to glance at the microwave. haha) The 31st of July is the Thriller’s birthday. Yay! What should we get him? I’ve no clue, but I need to get on it. It’s a scant week away.
The 31st of July is the Thriller’s birthday. Yay! What should we get him? I’ve no clue, but I need to get on it. It’s a scant week away.



{kind=link}
{kind=link}